First, I want to start out by saying that I do not know why it is called a MIC-KEY button, but I do know that there are other types of G-tubes out there, like the PEG, but the MIC-KEY is the one that Children's uses, and I have heard that it is 'better' then some of the others and easier to use. One of the differences that I have seen is the the MIC-KEY sits pretty flat on Hazel's tummy and the tube comes out the side whereas I think that the tube for the PEG comes straight out.
Next, I want to assure you that I am not a doctor. Or a nurse. Or anyone having anything to do with anything medical in any professional way. The only reason I know anything about any of this is through experience, asking questions (did I tell you that while Hazel was in the hospital Jimmy and I took this great marriage course in our church and when he was asked to write down my hobbies, he wrote 'asking questions' as one of them? Well, he did, and I do) and reading...a lot. Preemie book? The one that said 'don't read this book cover to cover because it will worry you too much'? Yeah. I devoured that one. That being said, anything that I say here, or anywhere actually, should never be taken as medical advice, and feel free to correct me (nicely, please!) or add to anything that I say.
Anyway, here we go:
G-tube stands for gastrostomy feeding tube, with 'gastro' indicating something having to do with the stomach, and 'stoma' meaning 'hole', so we have a tube that passes feed through a hole into the stomach.
In the pictures below, you can see a diagram of the basis of the button itself and the extension kit. The 'balloon' looking part that is what goes on the inside of Hazel's stomach. A tube starts right at the end of the balloon, passing through it, passing through Hazel's abdominal wall and ends with the 'button' that sits right on her skin. The flap in the picture that is down and to the right is what closes the hole when there is no extension tube connected to it so that her stomach contents don't come out, and the little pointer looking thing pointing up and to the left is where you connect a syringe to inflate or deflate the balloon, in our case with water, that is on the inside. The purpose of the balloon is to hold the tube and button in place both so that it doesn't come out, and so that it stays snug against the skin and doesn't leak.


This picture below is the packaging for Hazel's 'emergency' tube. It is sterile and ready to be used in case hers comes out. So far, we have not needed this, and I am hoping to never, ever need this. Even though the tissue that forms the hole where the tube passes through heals much like a hole for an earring while the tube is in, it is not like an earring in that if the tube comes out, it will heal very quickly, beginning to close in a matter or 30 minutes or so, and being impassable in about 24 hours. This is a good thing if you remove the tube because you no longer need it, but a not so good thing if it is pulled out accidentally. This package also shows the size of the tube that Hazel has. It is has a diameter labeled at '12 French', which I don't know why it is French, nor what that unit of measuring is, but the other size is 1cm, which indicates the length of the tube between the top of the balloon and the bottom of the button. Which means that Hazel's abdominal wall is 1cm thick. Now, you may think 'how can that be? The stomach does not lie that close to the skin, so how can the tube be only 1cm long?' Ahhh...good question! And one that has an answer that then greatly affects the way that we are able to feed Hazel. You see, when Hazel had her surgery, they did the surgery laproscopically by making a cut in her belly button and another in her abdomen where the button would go. Then they pulled her stomach out to the edge of her abdominal wall and passed the tube through the hole that they made there and inflated the balloon. That is why if the tube came out in the first 2 weeks or so, she would have needed surgery to put it back. The stomach would have gone back to its original location in the abdominal cavity. Now, however, the stomach is more permanently connected to the abdominal wall by the tissue that forms the hole where the tube passes.
So, how does this affect how Hazel eats? Well, imagine that you have a tiny tummy with an opening at the top where the food goes in when it comes through the mouth. There is a flap covering that hole that is supposed to let stuff in, but not out. In a preemie, and many term babies, too, for that matter, that flap is very underdeveloped and immature, and so it is floppy and doesn't close well. Now, take that tiny tummy and stretch it way off to the side and imagine what happens to the opening at the top. Right. It's stretched, too, which means that the floppy flap is even less effective at keeping food where it belongs in the stomach. Add to that the extra space that the balloon is taking up in that tiny tummy, and you can imagine that we have quite the compromised stomach capacity. That is why Hazel has a hard time nursing. While nursing, the milk flow is fast and fills her tummy faster than she can handle it. That is why when we hang her feeds, we have to run them over an hour, which is much longer than an average baby would usually nurse.

This is a close up of the end of the extension kit. This is the end that we attach the feed pump to. The white clip is a clamp that we use to clamp off the tube when it's not in use. If you don't clamp it, then if you open one of the ports, and Hazel has anything in her stomach and she cries or kicks her feet or tightens her abdomen in any way, the contents of her stomach will come out the open port. This can be good, if you are trying to get gas out of her tummy (she did not get a NISSIN, by the way, so she is able to burp, in case you are wondering. A NISSIN is a procedure that tightens the top of the stomach to help control reflux but makes you not be able to burp or throw up). If she is very gassy and can't bring up a burp, we have a very large syringe, that we take the plunger out of and attach to the open port so that her stomach contents can bubble up and with them, the gas. When she calms again, gravity takes the contents back into her stomach. But in any other case, you pretty much want to let what goes in, stay in.

This is the other end of the extension kit. It snaps into the button on Hazel's tummy and locks into place (hence the 'key' part of the name? Don't know...)

The milk that I pump is hung in this bag...
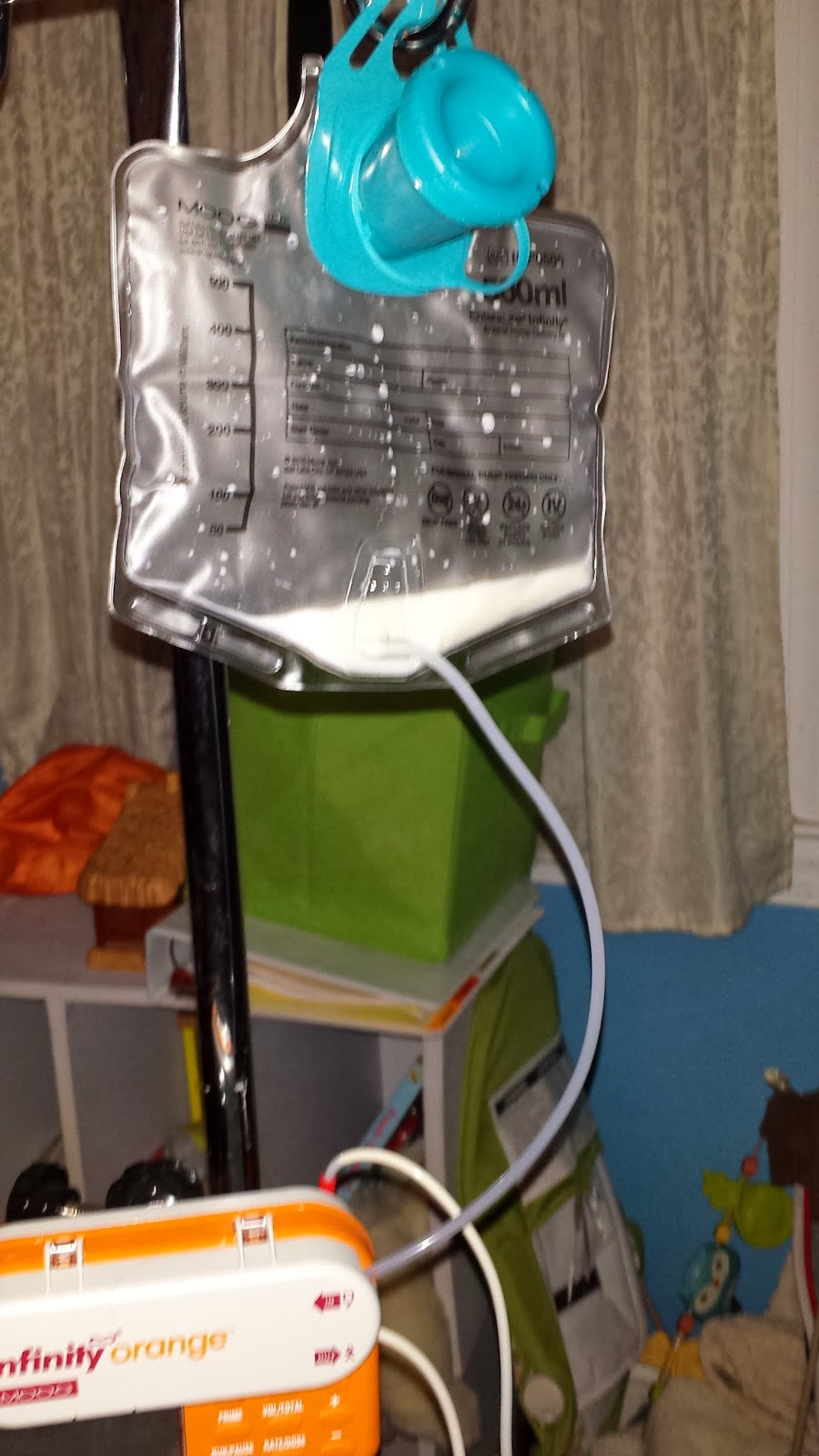
...and run through this pump.

Of course, you have to get the air out of the tubing before you can start the feed, so you can either use the 'prime' button on the machine, if you happen to have all day to wait for it, or you can squeeze the blue part of the tube where the little symbol of a drop of water is, squeeze the bag at the same time, and hope you don't squirt milk on the cat. Just sayin'. Things happen.

Then, the end of the tube from the feeding bag that has passed through the feeding machine is connected into the feed port of the extension kit like so,

the machine is programmed, and off we go!
The smaller port is where we put the medication in.
So, looking for the sliver lining in this whole thing, we have two very nice benefits that come from having a G-tube. One is that we never have to give Hazel her meds by mouth, we just push them through her tube, which is very handy when she has 4 oral meds she takes twice a day, and two, in the middle of the night, she just fusses a bit when she's hungry, and I have gotten quite adept at setting up her feeds quickly, and we both just fall asleep while they run and let the machine cut off when it's done.
Until, of course, she kicks her feet and happens to accidentally open the med port of a defective tube and we end up with a sopping wet mess of milk and stomach contents in her bed, but that doesn't happen often, thank goodness, and I have learned my lesson and I make sure to keep the tube up high and wrapped in a blanket so she can't kick at it.
And there you have it. That's how those cheeks have gotten so chubby!

No comments:
Post a Comment